


Focused Echo: Interpretation
Rationale.
Focused echocardiography is a systematic rapid assessment tool in the acute care setting.
The aim of focused echo is to provide a qualitative assessment of the overall cardiac function by answering specific simple questions (1). It also gives insight into the haemodynamic status, while being safer, faster and easier than other alternatives used with the same purpose, namely invasive central venous pressure (CVP) monitoring (2). Consequently, it’s an invaluable technique to assist the management of chest pain, dyspnoea, shock, and cardiac arrest. When combined with other POCUS modalities (lung, aorta, fast and leg veins) is useful in differentiating shock (3).
THE QUESTIONS?
Focused Intensive Care Echo (1) can help answer the following questions:
Is the LV dilated or significantly impaired?
Is the RV dilated or significantly impaired?
Is there pericardial effusion or tamponade?
Is there pleural effusion?
Is there evidence of low preload?
Are there any other obvious abnormalities?
CLASSIC HAEMODYNAMIC PATTERNS
Haemodynamically unstable patients can present with classic patterns identifiable by echocardiography. These patterns become more obvious and easy to detect as the clinical condition deteriorates:
Poorly contracting LV: Cardiogenic Shock.
Dilated RV, underfilled LV: Obstructive Shock (Pulmonary Embolism).
Pericardial fluid with RV collapse: Obstructive Shock (Cardiac Tamponade).
Vigorously contracting, underfilled LV: Hypovolaemic/Septic shock.
LIMITATIONS: FOCUSED VERSUS COMPREHENSIVE
Formal echocardiography is a comprehensive assessment that involves almost every morphologic and functional aspect of the heart. This skill can only be acquired with extensive formal training under expert supervision, which is outside the practical achievement of most emergency practitioners. When a thorough echocardiogram is required, a formal study should be arranged (4).
The focused approach is simpler and comprises two-dimensional (2D) images without most of the more complex quantitative measurements; hence, it is also easier to master. It has been shown that a rapid goal-directed, focused study can be carried out with a limited amount of training (5). Focused echo has the added advantage that the clinician carrying out the exam is also treating the patient and, thus, is best placed to relate the echo findings to the clinical situation (6).
Even when the general rule is that ultrasound may not delay resuscitation of a shocked patient nor obstruct the management of more pressing issues such as an unstable airway, it should be considered that bedside echo might be fundamental for optimal resuscitation before successful rapid sequence intubation.
Protocol.
Focused Cardiac Ultrasound, as a concept, has various names in the literature, and several academic groups have proposed different protocols (7-10). However, these may include assessments that are too complex for the bedside, not relevant in the acute setting, or incomplete. Furthermore, in emergency medicine, a widespread cardiac protocol (such as FAST for trauma) is still elusive.
FICE & 5E
The Focused Intensive Care Echocardiography (now FUSIC Heart) protocol (1) is sponsored by the British Intensive Care Society and widely accepted within the UK. Although dismissing the aortic root, it provides an adequate overall assessment of the cardiac function based on five simple binary questions:
Is the LV dilated or significantly impaired?
Is the RV dilated or significantly impaired?
Is there pericardial effusion or tamponade?
Is there pleural effusion?
Is there evidence of low preload?
The approach is simple enough to be adopted by Emergency Medicine practitioners, and more importantly, it contemplates a well-structured training process where at least 50 scans are required for sign-off and independent practice.
Alternatively, the 5E Protocol – Entrance, Ejection, Equality, Effusion, Exit (11) – is a standardised and easy-to-remember diagnostic tool with a conceptual framework similar to FICE, making it a good complement in the acute setting. 5E includes a basic assessment of the Aortic root (Exit), and a deeper analysis of preload and IVC (Entrance).
FICE + 5E
Entrance: is there evidence of low preload?
The IVC diameter changes depending on intravascular volume status, and normally, the IVC collapses during spontaneous inspiration. Therefore, the IVC diameter represents a non-invasive method for estimating central venous pressure (CVP). The evidence suggests that in spontaneously breathing patients, there is a good correlation between the sonographic estimation of CVP and values measured with invasive methods (2). IVC filling and CVP, however, allow only a rough correlation with volume status, and the sonographic estimation of preload should at least include the assessment of the LV and the Lung. Thus, it is better to think of IVC filling as an indicator of fluid tolerance, instead of a determinant of fluid responsiveness (6).
IVC exploration is best from the subxiphoid approach with longitudinal and transverse images. The IVC should be assessed in terms of overall size and collapsibility. The diameter is typically measured at its largest (end of expiration) at 1-2 cm distal to where the hepatic veins join the vena cava. An IVC diameter of ≥ 2 cm, especially with minimal or no collapsibility, is considered plethoric and correlates with increased RA pressure. An IVC of < 1 cm, particularly with complete collapse, is considered flat and indicates low preload and potential fluid responsiveness. An IVC diameter between 1 and 2 cm is typically normal.
-
![]()
Longitudinal
Following the IVC upwards will reveal the hepatic veins junction and the entrance to the RA. The Diaphragm can cause a mirror image of the heart.
-
![]()
Respiratory Collapse
The IVC diameter changes depending on intravascular volume status. The IVC collapse during spontaneous inspiration is normal.
-
![]()
Depleted
An IVC of < 1 cm, particularly with complete collapse, is considered flat and indicates low preload and tolerance to fluid challenges.
-
![]()
Plethoric
An IVC diameter of ≥ 2 cm, especially with minimal or no collapsibility (notice the absence of collapse in this clip), is considered plethoric and correlates with increased RA pressure.
PITFALLS
In a long-axis view, beware of not sliding off the centre of the vessel, as this will underestimate the size of the IVC and overestimate its collapse. Obtaining long and short axis views may help avoid this pitfall. Another mistake is confusing the descending aorta for the IVC, particularly when scanning in long-axis. Although the IVC may appear to pulsate, the aorta has a thicker wall, and its position is to the patient’s left. Following the IVC upwards will reveal the hepatic veins junction and the entrance to the RA, while the aorta will travel behind the heart. The IVC moves both anterolaterally and craniocaudally with inspiration, and this should be considered during visualization or measuring. For this very reason, measuring in M-mode is not recommended as it would not be accurate.
-
![]()
IVC Movement
The IVC moves both anterolaterally and craniocaudally with inspiration, and this should be considered when measuring.
-
![]()
IVC & Aorta
Don’t confuse the descending aorta for the IVC. The aorta has thicker walls and notorious abdominal branches.
-
![]()
IVC & Aorta
Although the IVC may appear to pulsate, the aorta has a thicker wall, and its position is to the patient’s left.
SHOCK
In a shocked patient, a flat or highly collapsible IVC correlates well with low preload estates (hypovolaemia, haemorrhage, sepsis). Yet by itself, a small IVC is not enough to define low preload and could also represent a normal finding.
Conversely, a distended, not collapsing IVC suggests distal obstruction in a shocked patient. Potential causes include LV failure, massive PE, tension pneumothorax and cardiac tamponade. Nonetheless, there are other causes of elevated cava / RA pressure, such as chronic pulmonary hypertension.
Accurate preload estimation requires clinical context and assessment of cardiac function:
If the IVC is flat, how is the LV managing the preload? Is the LV empty and hyperdynamic? If yes, then there is evidence of low preload.
If the IVC is non-collapsible, how is the RV and the LV managing the preload? Is the LV contractility impaired? is there evidence of obstruction to venous return?
Ejection: is the LV dilated or significantly impaired?
THE VIEWS
The PLAX view is versatile and allows the recognition of multiple landmarks, making it good for visual estimation of LV contractility. It is essential to optimize the view ensuring a true sagittal long axis, as being oblique to the LV chamber may underestimate its size and overestimate its emptying. The PSAX view at the level of the papillary muscles reveals the entire muscular circumference and concentric squeeze of the LV. It is useful to estimate both global function and focal wall motion abnormalities. The A4C view, although technically challenging, provides good insight into the global myocardial function and chamber size.
LV CONTRACTILITY
Qualitative assessment of the LV and visual estimation of Ejection Fraction is based on three parameters:
Endocardial excursion.
Myocardial thickening.
Movement of the anterior leaflet of the mitral valve.
A qualitative assessment is typically categorised as:
Normal (LVEF 50-65%)
Moderately Depressed (LVEF 30-50%)
Severely Depressed (LVEF < 30%)
Hyperdynamic (LVEF > 65%)
-
![]()
PLAX | Normal Contractility
You should already know the chambers. Now, explore the septum and LV free wall; notice the myocardial thickening and endocardial excursion. Appreciate the mitral valve activity and follow the movement of the anterior leaflet of the mitral valve
-
![]()
PSAX | Normal Contractility
In the short-axis view compare the size and shape of the chambers. Notice the homogenous concentric contraction of the LV.
-
![]()
A4C | Normal Contractility
In the apical view explore the size and shape of the 4 chambers. Notice the myocardial thickening and endocardial excursion. Appreciate the valvular activity and the rise of both tricuspid and mitral annulus.
-
![]()
SubXiphoid | Normal Contractility
Again, explore the myocardial thickening and endocardial excursion. The subxiphoid view gives a good insight into the overall contractile activity.
SIGNIFICANTLY IMPAIRED / DILATED LV
A severely depressed LV contractility, particularly when paired with a plethoric IVC or lung B-lines, indicates systolic heart failure. Chronically raised afterload can lead to severe dilation of the LV.
A “non-coordinated myocardial activity” can be recognised during cardiac arrest, and its prognosis is beyond poor.
-
![]()
PLAX | Severely Depressed
22 y/o Female with recently diagnosed miliary TB complicated with CAP. Quickly developed septic shock + cardiogenic shock secondary to sepsis and severe acidosis (pH 6.8). The patient required emergency RSI and suffered a post-intubation cardiac arrest, successfully achieving ROSC after 20 minutes of standard ALS resuscitation. These clips were taken after stabilisation in ICU, running an infusion of adrenaline + noradrenaline, and continuous renal replacement therapy.
-
![]()
PSAX | Severely Depressed
In this PSAX view, notice the severely poor circumferential contractility of the LV. The myocardium barely thickens.
In the previous PLAX image, despite the seemingly vigorous activity of the mitral valve (secondary to inotropic drugs), notice how the anterior leaflet of the mitral valve remains far from the septum, Likewise notice the LV free wall and septum barely thicken. -
![]()
A4C | Severely Depressed
This A4C image is slightly off-axis (ballooned). Nonetheless, again notice the poor opening of the mitral valve and how the septum and LV free wall contract (thicken) poorly.
-
![]()
SX | Severely Depressed
In this sub-xiphoid view, notice the overall depressed contractility of the LV. There is also a small amount pf fluid adjacent to the RV.
-
![]()
IVC | Plethoric
The IVC is plethoric and shows no variability (IPPV). This is also in keeping with the diagnosis of cardiogenic shock, as the retrograde congestion affects the pulmonary circulation (cardiogenic pulmonary oedema) and increases the RA pressure.
-
![]()
PLAX | Severely Depressed
58 y/o Male. Background of dilated cardiomyopathy with an ICD in situ. Admitted to ICU in the context of acute heart & respiratory failure.
In this PLAX view notice the overrall poor cardiac activity and the severely dilated LV and LA chambers. Again the anterior leaflet of the mitral valve displays poor activity and opening. -
![]()
PSAX | Severely Depressed
PSAX view demonstrating a severely depressed contractility. The septum and LV wall barely thicken.
-
![]()
A4C | Severely Depressed
Notice the degree of chamber dilation and the overall reduced contractility. The ICD wire is visible within the RV.
-
![]()
SX | Severely Depressed
Notice the degree of chamber dilation, the thin walls and the overall reduced contractility. The ICD wire is visible within the RV.

-
![]()
PLAX | Severely Depressed
59 y/o Male with a background of dilated MCP and a mechanical mitral valve. Admitted to ICU with septic shock. Clips were taken with a running infusion of norepinephrine + dobutamine.
In this PLAX view notice the septum attempts to contract but the thickening is poor. The same is true for the LV free wall, there is movement but the contractile activity is severely reduced. -
![]()
PSAX | Severely Depressed
In this short axis view some degree of myocardial excursion is visible but severely abnormal and weak.
-
![]()
A4C | Severely Depressed
Assess the overall dilation of the cambers and poor contractility. The movement and artefacts caused by the mechanical mitral valve are also noticeable.
-
![]()
SX | Severely Depressed
Notice the overall dilation of the cambers and poor contractility. The LV walls do not come together and the walls are thin. The movement and artefacts caused by the mechanical mitral valve are also noticeable.
-
![]()
IVC Plethoric
Plethoric IVC (>2cm) and without respiratory changes.

HYPERDYNAMIC
In contrast, hyperdynamic states are associated with decreased afterload and are classically found in patients with sepsis or severe hypovolaemia. A hyperdynamic heart should be accompanied by a small, collapsing IVC. Moreover, is essential to remember that tachycardic is not the same as hyperdynamic, as the latter is a measure of contractile activity and emptying. A tachycardic heart is not necessarily hyperdynamic.
-
![]()
PLAX
51 y/o Female, admitted to ICU with septic shock, receiving ABX and norepinephrine. Spontaneous ventilation.
Despite the poor quality of the images, assess the increased contractile activity. There is a noticeable myocardial excursion and the LV walls come closer together. -
![]()
PSAX
Again, despite the poor quality of the images, notice the increased myocardial excursion and how the LV walls come close to each other. The RV is small (empty).
-
![]()
A4C
Notice the overall increased contractile activity and the active opening of the mitral valve.
-
![]()
SX
Notice the overall increased contractile activity. There is an increased movement and thickening of the LV wall.
-
![]()
IVC
The IVC is small (<1.5 cm) and fully collapses on spontaneous inspiration, correlating with a low preload and RA pressure.

-
![]()
PLAX
63 y/o Female, assessed in the ED with suspected sepsis. VBG with acidosis and rising lactate.
Despite the poor quality images, notice how the septum and LV free wall actively move, thicken and virtually touch each other. -
![]()
PSAX
The same in this short axis view, there is increased contractility and excursion of the LV myocardium. The RV is small and empty.
-
![]()
A4C
Notice the overall increased contractile activity of the LV.

-
![]()
PLAX
21 y/o Female, assessed in ED with low GCS, agitation, hypotension & metabolic acidosis. Oral mucose and skin appear severely dry on examination.
In this PLAX view, observe the “small” size of the chambers and the active opening of the mitral valve anterior leaflet, touching the septum. Notice the exaggerated excursion of the septum and LV free wall, both thicken to almost kiss each other. -
![]()
PSAX
The increased myocardial excursion is rather noticeable in this short axis view at the level of the papillary muscles.
-
![]()
IVC
Despite the poor quality of the clip, the IVC is small and fully collapses on spontaneous inspiration.
PITFALLS
While distinguishing normal function from severe dysfunction might be easy, moderate LV depression is more difficult to reliably discern. Also, it should be noted that even with a preserved ejection fraction, heart failure still remains a possible cause of dyspnea. A big percentage of heart failure cases have some component of impaired relaxation, leading to diastolic dysfunction, or heart failure with preserved ejection fraction.
-
![]()
Moderately Deppressed
49 y/o Female, admitted to ICU with dyspnoea and acute heart failure. No CHF background. The working diagnosis was a suspected Takotsubo syndrome and a formal echo performed after these images measured an EF of 35%-40% (moderate dysfunction)
-
![]()
Moderately Deppressed
-
![]()
Moderately Deppressed
Both in this apical view and the PLAX view, notice how the contractility is globally reduced but worse towards the apex, exhibiting poor apical myocardial excursion.
E-POINT SEPTAL SEPARATION
Active movement of the MV anterior leaflet during diastole, so it nearly touches the septum, correlates with good LV filling and ejection fraction. This can be assessed objectively by measuring the E-point septal separation (EPSS), which is the distance between the septum and the mitral anterior leaflet either in B-mode or M-mode. EPSS < 7mm is considered normal. EPSS is a good surrogate measure of ejection fraction, but it should be used with caution, as septal hypertrophy and mitral valve stenosis can lead to wrong estimations. In the PLAX view, it is important to have the septum lying horizontally flat on the image, as an oblique orientation may result in an overestimation of the EPSS.
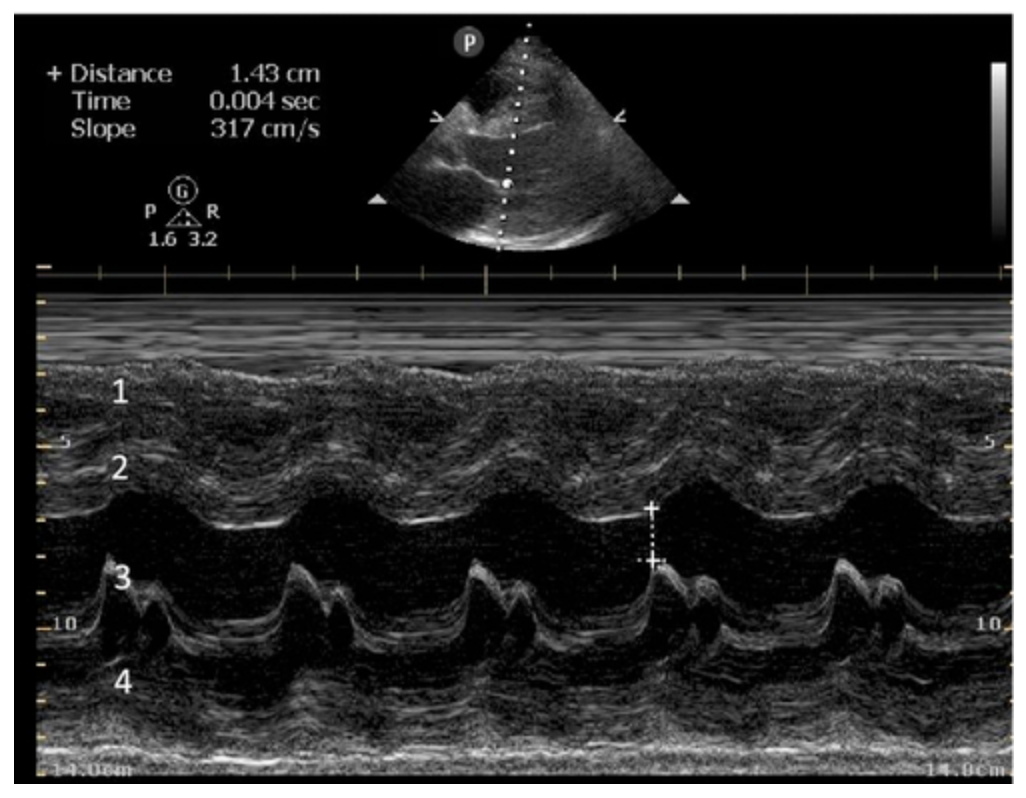
Depiction of E-point septal separation: M-mode is used to measure the distance between the open mitral valve and the ventricular septum. Measurements greater than 7 mm are suggestive of depressed systolic ejection. (1. RV free wall, 2. Interventricular septum, 3. Mitral valve, 4. LV free wall). From: The "5Es" of emergency physician-performed focused cardiac ultrasound (11).
-
![]()
PLAX 17cm
68 y/o Male with a background of cardiac sarcoidosis admitted to ICU with respiratory failure (IPPV), persistent hypotension requiring vasopressors, and new LBBB + raised troponins.
Notice there is some myocardial thickening but the overall LV contractility is significantly depressed. Likewise, the mitral valve movement is poor. -
![]()
EPSS
M-Mode represents exclusively a small linear section of the 2D image (Upper image: thick grey vertical line in the middle of the screen) perpetually updated across time. Below, the horizontal “wavy” middle line is the movement across time of the anterior leaflet of the mitral valve. The EPSS, measured between the open mitral valve and the septum is >7mm (1.08cm) and, therefore, abnormal.
-
![]()
PLAX 21 cm
This clip highlights how adjusting the depth is useful. Notice that at 21 cm depth, you can more easily visualise the descending aorta.
Also, the presence of a left pleural effusion and lung consolidation adjacent to the LV free wall becomes evident. -
![]()
PSAX
The circumferential contractile activity of the LV is significantly reduced.
-
![]()
A4C
There is reduced global contractility of the LV. The chambers are not significantly dilated
-
![]()
SubXiphoid
There is reduced overall contractility of the LV and the chambers are not significantly dilated. There is a small but noticeable pericardial effusion adjacent to the RV & RA.
-
![]()
IVC
Plethoric, full IVC (>2 cm). There is no respiratory variability (IPPV).
-
![]()
Left Chest
Abundance of diffuse pathologic B-lines bilaterally.
-
![]()
Right Chest
Abundance of diffuse pathologic B-lines bilaterally.



Equality: is the RV dilated or significantly impaired?
Normally, the RV is a low-pressure, thin-walled, high-compliance chamber that wraps anteriorly around the muscular, cone-shaped LV. The normal RV : LV diameter ratio is 0.6 : 1.
When the pulmonary artery pressure rises, the RV will dilate, altering the normal RV:LV ratio. Although sacrificing sensitivity, the use of equality (1:1 ratio) as a cutoff can achieve a specific estimation of RV strain. If imaged correctly by a trained operator, the presence of an RV:LV ratio > 1 is highly specific for RV strain.
RV dilation can be acute, chronic, or acute-on-chronic. However, in patients presenting with undifferentiated chest pain, shortness of breath, hypotension or syncope, the presence of any RV dilation should raise suspicion for acute pulmonary embolism (PE). Furthermore, in a patient in shock, the presence of RV strain may signal the need for aggressive therapy – emergency thrombolysis.
THE VIEWS
The A4C view provides an accurate chamber size comparison. However, achieving a proper A4C view (avoiding foreshortening or ballooning, and visualising the four chambers with a vertically oriented interventricular septum) can be a challenging exercise of image acquisition. Additionally, the PSAX view at the level of the papillary muscles shows both LV and RV side by side and is useful to assess function and size. When RV pressure is high, the septum will be pushed and flattened towards the LV, resulting in the characteristic “D-shaped” LV or “D sign”.



-
![]()
PLAX
49 y/o Female who presents with severe respiratory distress and desaturation to 90%. Suspecting an airway obstruction secondary to a known thyroid mass, she’s been intubated in ED, after which the SpO2 has not improved and she’s become severely hypotensive requiring vasopressor support.
This PLAX view shows a hyperdynamic LV. There’s also a somewhat enlarged RV when compared to the LA and aortic root, breaking the 1:1:1 rule.
-
![]()
PSAX
The short axis view reveals a clearly flattened septum and a D-shaped LV.
The RV is at least the same size as the LV if not larger. -
![]()
A4C
This apical view demonstrates a massively dilated RA. The RV appears dilated in comparison to the LV; however, the RV free-wall is not well characterised in this clip so it is difficult to say more about it.
When this happens, small adjustments might improve the image. -
![]()
Massive PE
This improved view demonstrates a significantly dilated RV with septal deviation to the left. Notice the akinetic RV free wall and the ‘apical wink’ at the RV tip; both these findings constitute the McConnell's sign.
The patient received emergency thrombolysis with immediate correction of the hypotension and shock. You can find the full case in detail including CT images here: https://ultra-sono.com/cases/airwayobstruction
-
![]()
SX
SubXiphoid view demonstrating the massively dilated right chambers.
-
![]()
IVC
Significantly plethoric IVC with no respiratory variation or compressibility.

-
![]()
Cor Pulmonale
59 y/o Male with severe ARDS and a prolonged period of mechanical ventilation.
-
![]()
D Sign
Short axis view with D-shaped septum and dilated RV.
-
![]()
Cor Pulmonale
Severely dilated right chambers. The US scan for DVT was negative rasing the presumption of sub-acute Cor Pulmonale in the context of raised ventilatory pressures.
-
![]()
Cor Pulmonale
SuXiphoid view with severely dilated right chambers.
PITFALLS
When comparing size, beware of correct image acquisition, as oblique planes lead to misinterpreting the RV:LV ratio. For apical views be sure to slide the probe sufficiently laterally on the chest wall so that it lies over the true apex. Also, be sure to obtain a real horizontal plane, avoiding foreshortening (ballooning). For the PLAX view it is useful to fan through the heart’s long axis, making sure that LV visualization is maximized relative to the RV. Furthermore, an understanding of probe placement and marker orientation conventions is fundamental. If inadvertently scanning in reverse orientation, the normally larger LV could be mistaken for an abnormally enlarged RV.
-
![]()
PLAX
33 y/o Female presents to ED with acute dyspnoea. On assessment, there is a raised D-dimer and the following clips.
-
![]()
PSAX
-
![]()
A4C
-
![]()
SX
-
![]()
IVC

-
![]()
A4C
19 y/o Male. Suffered cardiac arrest secondary to a massive PE and subsequent ROSC. Thrombolysis was withheld as sustained a significant head injury.
These clips were taken 24 hours post-admission with the patient haemodynamically stable and ventilating spontaneously.
A4C demonstrates evidently enlarged RV (equal size to LV or 1:1). Notice, however, that the rest of the views are only suggestive but don’t categorically show an enlarged or abnormal RV. This highlights the value of the apical view for chamber size comparison and the importance of performing a full study before reaching any conclusions.
-
![]()
SX
-
![]()
PLAX
-
![]()
PSAX

Effusion: is there a pericardial or pleural effusion?
Pericardial effusion is a continuum and can potentially evolve into haemodynamic collapse. Tamponade physiology is detectable earlier with ultrasound than with traditional physical examination, and it has been demonstrated that PoCUS improves mortality in penetrating cardiac trauma. Timely and accurate diagnosis is, therefore, vital.
THE VIEWS
The subxiphoid view is the most reliable for detecting pericardial effusion. Still, it is ideal to obtain different views not to miss a focal effusion as small amounts of fluid can lead to tamponade physiology. Tamponade does not link strictly to the size of the effusion, but correlates more with the speed of onset, causes, and haemodynamic effects.
-
![]()
SX
Small pericardial effusion adjacent to the RV.
-
![]()
A4C
Small apical pericardial effusion
-
![]()
PLAX
52 y/o Male admitted to.a medical ward in the context of pleural effusion and suspected autoimmune disease.
PLAX shows a small to moderate pericardial effusion.
-
![]()
PSAX
Short axis view shows a moderate amount of fluid surrounding both ventricles.
-
![]()
A4C
Small to moderate pericardial effusion. There is no evident right chamber collapse in this view.
-
![]()
SX
Moderate pericardial effusion.
The RV contracts during ventricular systole and re-expands during ventricular diastole, there is no diastolic collapse of the RV. This is normal and rules out tamponade.
The RA empties (collapses) during ventricular diastole and fills (re-expands) during ventricular systole. There is no systolic collapse of the RA. This is normal and rules out tamponade.
-
![]()
IVC
The IVC is < 2 cm and presents some degree of inspiratory collapse.
-
![]()
PLAX
33 y/o Female with a background of diffuse B-cell lymphoma. Admitted to a medical ward with progressive legs and facial oedema, bradypsychia, lethargy and cold intolerance. TFT was compatible with hypothyroidism.
PLAX shows a moderate to large amount of fluid surrounding both ventricles and causing a “swinging heart”.
-
![]()
PSAX
There is a moderate to large pericardial effusion surrounding both ventricles and causing a swinging motion with each contraction.
-
![]()
A4C
Moderate pericardial effusion. There is no evident RV diastolic collapse.
-
![]()
SX
Moderate pericardial effusion. There is no evident RV diastolic collapse.
PITFALLS & PLEURAL EFFUSIONS
A common error is to confuse a pericardial fat pad with effusion. Fatty tissue has a heterogeneous echotexture, moving in coordination with the myocardium, and it cannot be tracked around the heart, especially posteriorly and to the apex. Another pitfall is misinterpreting a pleural effusion as a pericardial effusion. However, they can be differentiated by their relationship to the descending aorta. Pericardial effusion may be seen between the aorta and the LV free wall, whereas pleural effusions are posterior to the descending aorta. Lastly, other causes, namely hypovolaemia and large pleural effusions, can cause RA and RV collapse.
-
![]()
Pleural or Pericardial Effusion?
-
![]()
Pleural or Pericardial?

-
![]()
PLAX
56 y/o Male. Background of cirrhotic liver disease. Admitted to ICU with UGIB complicated with respiratory sepsis.
Pleural effusion on PLAX. The fluid tracks behind the descending aorta.
-
![]()
A4C
Apical view. Left pleural effusion, lung consolidation & B-lines adjacent to the LV.
-
![]()
Left Lung Base
Pleural effusion accumulated on the left costophrenic angle. See the consolidated lung floating within the fluid.
-
![]()
Right Lung Base
Pleural effusion and large organised consolidation of the right basal zone of the lung. The dense structure that resembles the liver is the hepatised lung with air bronchograms (the bright white bits within). Although a hepatised lung resembles the liver the aspect is not identical, compare this to the next image.
-
![]()
Abdominal Right Upper Quadrant
There is an abundance of ascitic fluid. The liver is slightly more homogenous in aspect than the hepatised lung of the previous clip.
-
![]()
PLAX
PLAX view with severely depressed LV contractility. There is a pleural effusion adjacent to the LV. Increasing the depth would be an ideal way to assess this i more detail.
-
![]()
PSAX
Fluid collection located outside the pericardium in short axis view
-
![]()
SX
Fluid collection adjacent to the RV but outside the pericardium. Notice the consolidation within this pleural effusion and some protein organization of the fluid. There is also an ICD wire within the RV.
-
![]()
A4C
Lung consolidation adjacent to the RV
CARDIAC TAMPONADE
Progressively rising pressure translates into evolving tamponade, and this accompanies a series of ultrasound findings:
Initially, the RA collapses during ventricular systole (closed AV valves).
Followed by RV collapse in ventricular diastole (open AV valves).
Ultimately leading to LV collapse.
In addition, the presence of a non-collapsible, plethoric IVC is one of the most sensitive signs of tamponade, and a finding easy to visualise. Conversely, a pericardial effusion in a haemodynamically stable patient with a collapsible IVC is unlikely to represent tamponade.
Chamber collapse can be assessed in M-mode, where the collapsing RV is seen as a notch that takes place right after the mitral valve opening and before its closure (during diastole).

M-mode is used to demonstrate RV collapse (arrow) occurring right after mitral valve opening during diastole. (star = pericardial effusion, 1. RV free wall, 2. Interventricular septum, 3. mitral valve, 4. LV free wall). From: The "5Es" of emergency physician-performed focused cardiac ultrasound (11).



Exit: is there acute aortic root pathology?
Thoracic Aortic dissection is a time-dependent and deadly pathology that can occur silently or be masked by a variety of clinical presentations. While angio-CT remains the gold standard for diagnosis, US may be performed quicker and at the bedside. In the visible portion of the aortic root, the US findings can include intimal flap, aortic valve insufficiency, retrograde aortic flow, or rupture into the pericardium with pericardial effusion and tamponade. Alternatively, dilation of the aortic root is characteristic of a thoracic aortic aneurysm.
Importantly, remember that thoracic aortic dilation or intimal flap may occur distal to the aortic root, where an US scan is usually blind. Hence, the absence of dilation or flap does not rule out aortic disease.
THE VIEWS
The PLAX view is best for exploring the aortic root. If performed by an experienced operator, aortic root measurements in this window correlate well with angio-CT measurements.
The Aortic root size varies with age and gender and should be measured at its widest point, perpendicular to its long axis. In general, a root > 4 cm should be considered borderline and enough to warrant a formal study.
Alternatively, the aortic root size can be estimated by the rule of thirds, where in the PLAx view the size of the RV, AoR, and LA should be roughly 1:1:1.
-
![]()
1:1:1
In the PLAX view, the sizes of RV, AoR, and LA are roughly 1:1:1. This is Normal.
-
![]()
Dilated Aortic Root ?
In this PLAX view, the AoR appears slightly larger than the RV and LA. A formal Echo identified a 39 cm AoR and was considered normal for the patient’s demography.
-
![]()
Aneurysmatic Aortic Root
This PLAX view shows and evidently enlarged AoR, measuring 5 cm. The 1:1:1 rule is not respected. There are no obvious signs of complication in this clip.
-
![]()
Aneurysmatic Aortic Root
AoR 5cm transversal diameter.

-
![]()
Normal Aortic Arch
A suprasternal view can be used to explore beyond the aortic root towards the arch and the emergence of its branches. The probe is placed in the supraesternal notch pointing caudally and with the marker oriented to the left ear.
(BCA: Brachiocephalic Artery. LCA: Left Carotid. LSA: Left Subclavian. DA: Descending Aorta) -
![]()
Aneurysmatic Aortic Root
Suprasternal notch view of the same patient in the previous set (5cm AoR). This view is not the best to measure as anatomy is slightly distorted. Notice, however, that the inner wall definition is adequate and, if present, it could demonstrate a dissection flap.
-
![]()
Aortic Arch
Same patient. Fine probe adjustment allows further exploration of the Ao Arch.
AORTIC DISSECTION
In both of these views, US may detect an intimal flap seen as a hyperechoic linear structure within the aortic lumen that moves with each heartbeat. The visualization of a flap carries a high specificity and should prompt immediate consultation with cardiothoracic surgery; however, ultrasound sensitivity for intimal flap is significantly low, and its absence does not rule out aortic dissection.
Author: Felipe Urriola-Perez | Review: Pablo Extremera-Navas
Published: 08.12.23
Reference.
FUSIC Heart Training Pathway. Intensive Care Society. https://ics.ac.uk/product/heart.html
Ciozda, W., Kedan, I., Kehl, D.W. et al. The efficacy of sonographic measurement of inferior vena cava diameter as an estimate of central venous pressure. Cardiovasc Ultrasound 14, 33 (2015). PMID: 27542597
Weingart, SD. The RUSH Protocol https://emcrit.org/rush-exam/original-rush-article/
Bowra, Justin; McLaughlin, Russell; Atkinson, Paul; Henry, Jaimie. Emergency Ultrasound Made Easy, Third Edition. 2022. Elsevier Health Sciences.
Randazzo MR, Snoey ER, Levitt MA, Binder K. Accuracy of emergency physician assessment of left ventricular ejection fraction and central venous pressure using echocardiography. Acad Emerg Med. 2003 Sep;10(9):973-7. PMID: 12957982
Basaure, Carlos; Clausdorff, Hans; Riquelme; Felipe. Ultrasonido Clínico, First edition. 2018. Emergency Medicine Residency Program, Universidad Católica de Chile.
Spencer KT, Kimura BJ, Korcarz CE, Pellikka PA, Rahko PS, Siegel RJ. Focused cardiac ultrasound: recommendations from the American Society of Echocardiography. J Am Soc Echocardiogr. 2013 Jun;26(6):567-81. doi: 10.1016/j.echo.2013.04.001. PMID: 23711341.
https://www.winfocus.org/course/basic-echocardiography/
Aleksandar N Neskovic and others, Focus cardiac ultrasound core curriculum and core syllabus of the European Association of Cardiovascular Imaging, European Heart Journal - Cardiovascular Imaging, Volume 19, Issue 5, May 2018, Pages 475–481, https://doi.org/10.1093/ehjci/jey006
https://www.resus.org.uk/training-courses/adult-life-support/feel-focused-echocardiography-emergency-life-support
Kennedy Hall M, Coffey EC, Herbst M, Liu R, Pare JR, Andrew Taylor R, Thomas S, Moore CL. The "5Es" of emergency physician-performed focused cardiac ultrasound: a protocol for rapid identification of effusion, ejection, equality, exit, and entrance. Acad Emerg Med. 2015 May;22(5):583-93. PMID: 25903585